Pathophysiology of Human Immunodeficiency Virus (HIV)
3 comments
Hello and Good day, it is a pleasure to be writing another post to the beautiful post on this community. Before I begin my post today, let me tell you a short story. I was outside with a friend, and we went to the laboratory to get a full test. When I was at the laboratory, I told the attendant that I wanted a full test, and the person beside me said the same thing and then said he didn't ask to be tested for HIV. I was surprised, who goes for a full blood test and omits HIV? He said he didn't want to have a death sentence in writing when he still had a long life to live. He preferred not knowing his HIV status so he can be happy, rather than knowing he is positive and starting to think. Let me say clearly that being HIV positive isn't a death sentence, just ensure you speak to your medical counselor and use the retroviral drugs prescribed to you. This said I guess you already have a glimpse of what I will be discussing tonight. I will be discussing the Human Immunodeficiency Virus (HIV) extensively.
The Human Immunodeficiency Virus (HIV) is a retrovirus that infects the CD4 T-cells. CD4 (cluster of differentiation 4) is a protein found on the surface of certain types of white blood cells, including T helper cells, monocytes, and macrophages. They are important in helping to coordinate and direct immune responses. When it infects the CD4 T-cells, it destroys them causing impairment in cell-mediated immunity and increasing the risk of its host being infected by opportunistic pathogens and risk of cancer. When I talk about HIV, it is good to know that there are two species which are HIV-1 and HIV-2. HIV-1 is the most common type of HIV in the world, and HIV-2 is basically common in West Africa.
commons.wikimedia.org
{kind=link}
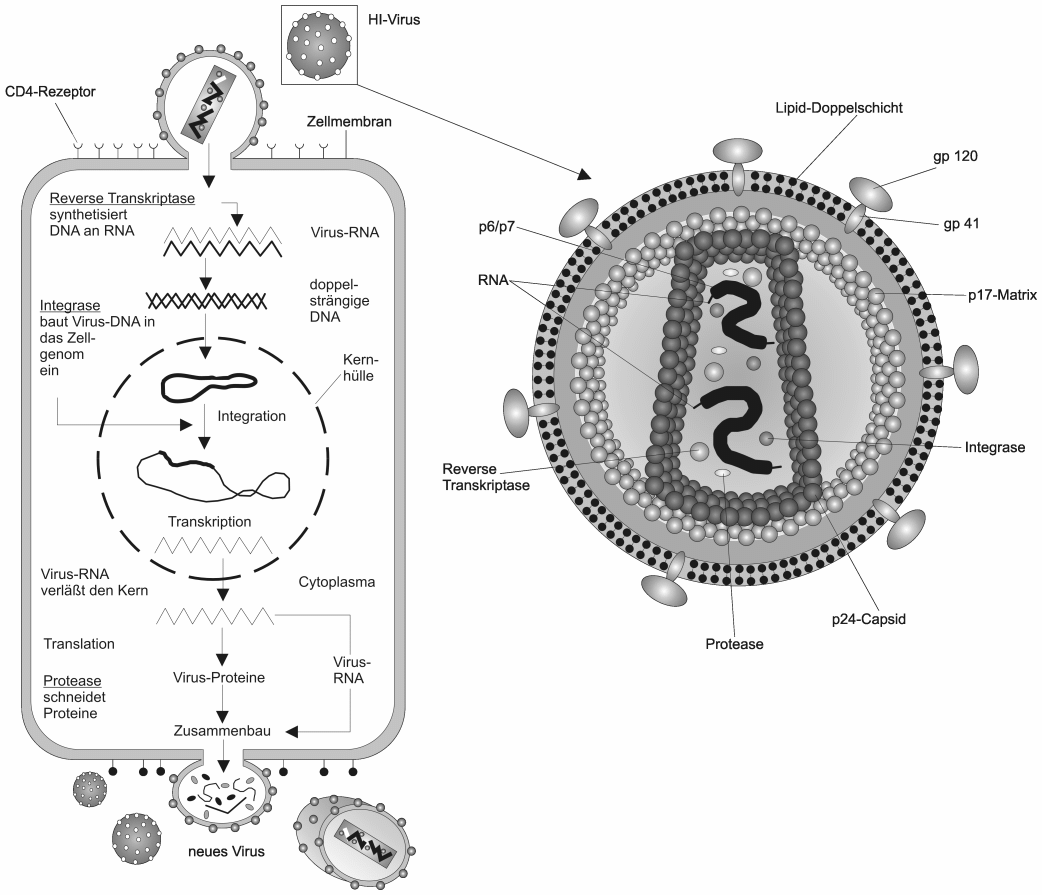
HIV is an Icosahedral-shaped virus with a conical capsid (protein shell). The capsid of the Virus has two RNA strands which are made up of 9 genes responsible for holding the genetics of the Virus and has two enzymes, the Integrase, and Reverse Transcriptase which are essential for its replication. The genes in the RNA of HIV contain the instruction for multiplication. CAG, POL, and ENV provide instructions which are the core protein, enzymes, and envelope which are covered with glycoprotein spike, to form the virus particles after multiplication. The glycoprotein helps the virus to stick to the CD4 T-cell receptor.
HIV gets into the cell through sexual intercourse (which is the major cause) through semen and vaginal fluids, parentally through blood, and vertical transmission through breast milk from mother to baby. When the virus gets to the body, the infects the immune cells with CD4 receptors in the body. When they reach the cell, the GP120 spike on the virus attaches to the CD4 receptor, and chemokine co-receptors CCR5 receptor, and CXCR4 receptor of the cell, causing the membrane of the virus to fuse to the cell membrane of the Lymphocyte. When the virus-cell attaches to the cell membrane, it begins fusion where the HIV capsid enters the CD4 cell. In this stage, the GP41 of the HIV virus fuses the HIV envelope to the cell wall after which the virus RNA (the reverse transcriptase and the integrase) is released. After the fusion, the next step is reverse transcription where the reverse transcriptase enzyme is used to convert the RNA into pro-viral DNA in the cell called cDNA. After reverse transcriptase, the next step is integration where the viral cDNA uses the host's enzymes to integrate itself into the host cell's chromosomes. Integration is a critical step in the HIV replication cycle as it allows the virus to evade the host's immune system by hiding its genetic material within the host cell's genome. It also ensures that the viral genetic material is passed on to any new cells that are produced when the host cell divides. In this stage, the HIV integrase enzyme attaches itself to the end of the proviral DNA strand where it takes the viral DNA into the cell nucleus where it attaches to the host DNA. At this stage, it can either remain dormant within the cellular DNA known as Latency, or it can use the host's cell machinery to replicate. The next step is known as transcription where the cell becomes active, and the virus uses the host enzyme RNA Polymerase to make mRNA and genomic viral RNA. The next step is known as translation, where the mRNA and the host enzyme begin to assemble into new viruses at the cell wall, after which the newly created virus pushes out of the cell wall of the virus. The cell wall of the new virus will contain lipids that make its surface glycoprotein including the gp120 and gp41. After being released from the cell, the viral protease cleaves to precursor proteins which help in forming matured capsid which allows it to be infectious. This cycle continues.
When a person gets infected by HIV, the dendritic cells which are a type of immune cells that identifies capture, and present antigens to other immune cells, first recognize the HIV virus and present them to the Immune system, where the lymph nodes engulf the virus and present them on the cell surface with the help of major histocompatibility complex class II (MHV class 2). The virus travels to the Gut gastric associated lymphoid tissue where CD4 T-lymphocytes are activated. The CD4 T-cells activate the cytotoxic T- cells (CD8 T-cells). At this point, HIV infects the CD4 receptor cells which are the Macrophages, monocytes, microglia, T-lymphocytes, and dendritic cells. As they replicate, they kill the cells and spread increasing the viral load. At this point, the HIV P24 antigen becomes detectable and the HIV antibodies begin to show. This process is known as seroconversion, causing seroconversion sickness which includes fever, myalgia, fatigue, rash, lymphadenopathy headache, and pharyngitis. As HIV keep evading CD4 T-lymphocyte and multiplying, their genetic material keeps mutating preventing them from being destroyed by the immune system. For 10 years, HIV symptoms can be asymptomatic, as the virus remain dormant in the CD4 T-cell, and the viral load remains the same and are detectable. When the CD4 cell count is low (below 200 cell count), a person with HIV is at risk of developing AIDS.
Diagnosis of HIV can be done through a Combination Assay, where the presence of P24 antigens and HIV antibodies are viewed. A differentiation Assay can be done to tell the type of HIV the person is infected with. Also, the HIV viral load can be checked using HIV RNA nucleic acid amplification test (NAAT). Treatment of HIV includes Anti-retroviral therapy which is a lifelong treatment. Management includes education on safe sex, the ability to live a normal life when taking treatment, and complications of the disease.
Comments