A Case of Microcystic Stromal Tumor
10 comments
Microcytic Stromal Tumor is an ovarian stromal tumor with distinctive microcystic appearance (WHO definition at the time of this writing). This was a case of a 53 year old female who complained about a pelvic mass on her right.
Note: It's been a while since I posted from this account. One thing I want to point out is I don't format my posts in a casual show and tell. Not for academic purposes. The images here are my own photos. I recommend further readings about the subject as not everything here is covered about the case.
Usually affecting only one of the ovaries which is what is present in the case and measuring around 6.5cm wide.
It's predominantly solid, firm, tan-white with focal areas of hemorrhage.
Here's an image of the actual specimen:
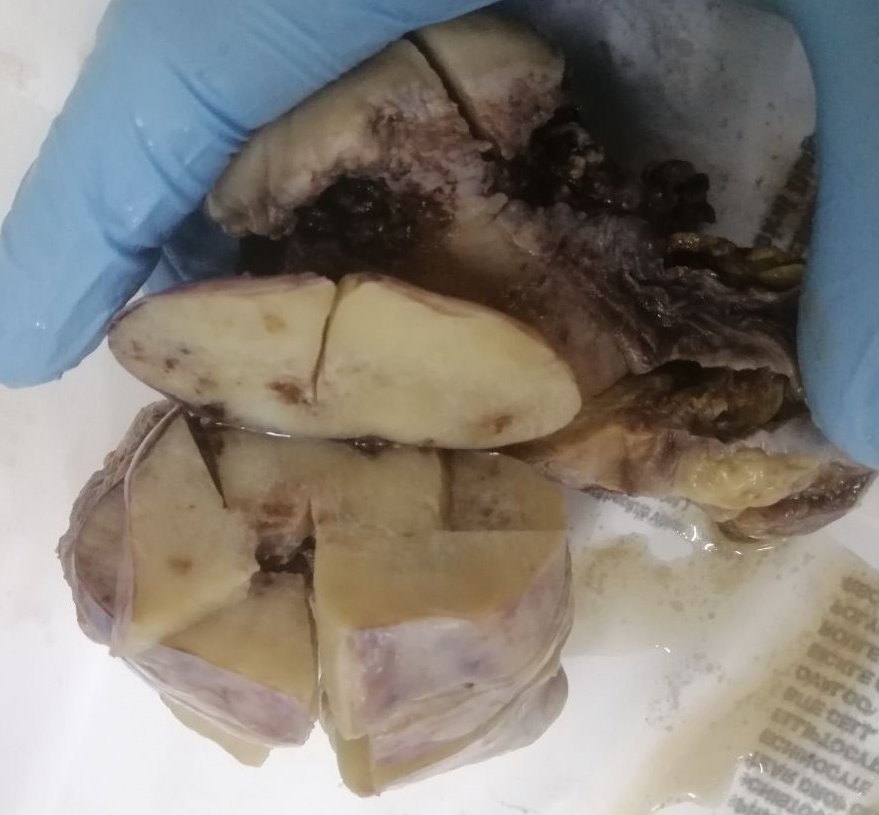
Though it's not really obvious from this angle but this is a right ovary, enlarged and converted into a tumor. The background is a uterus and cervix but it's hard to tell from this point of view. I didn't really document the grossing because I thought it was just a case of ovarian fibroma. Well I don't work on cases thinking I could blog this stuff as an initial reaction.
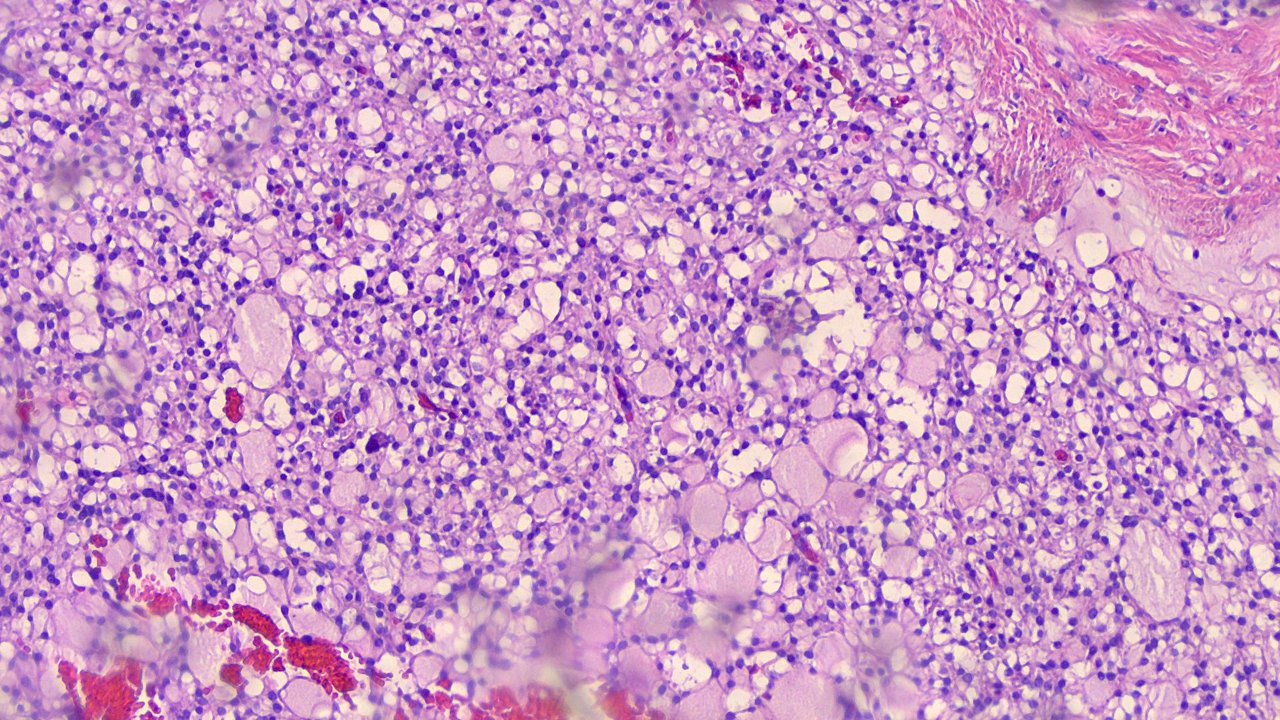
Taken at scanner view (40x magnification):
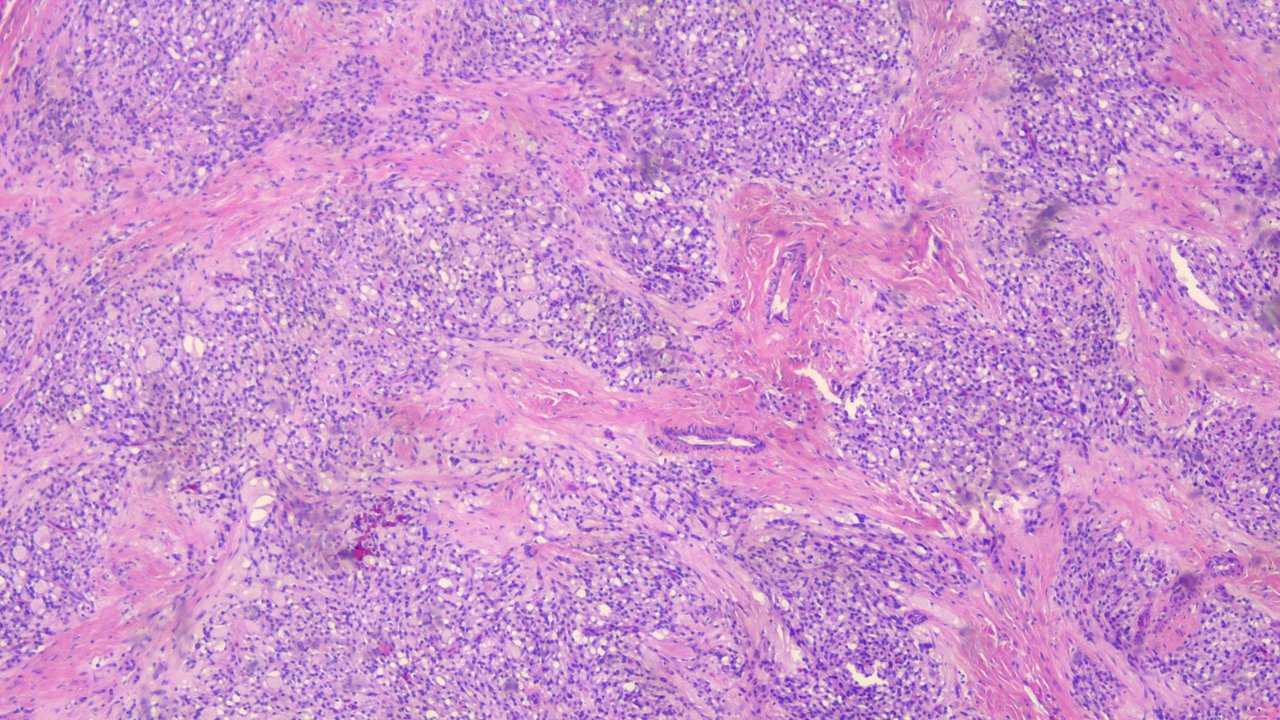
There are three things notable about this tumor:
- Microcysts.
- Solid cellular zones
- Fibrous stroma.
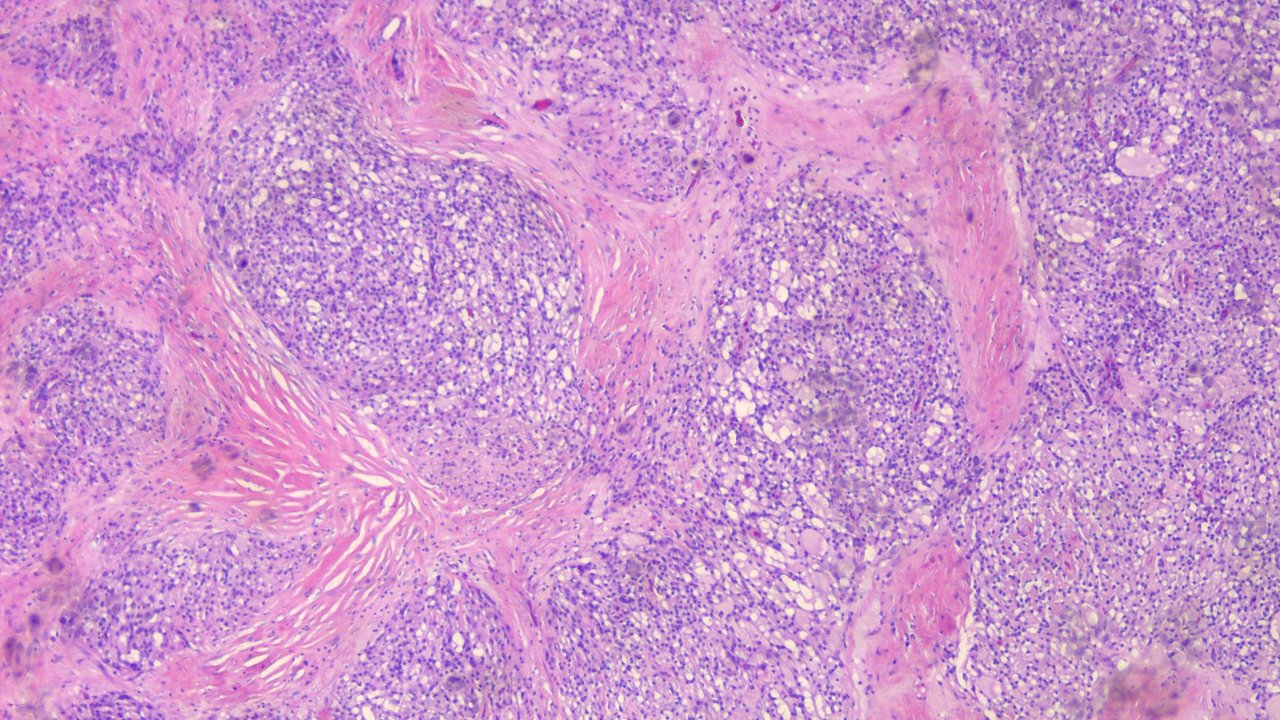
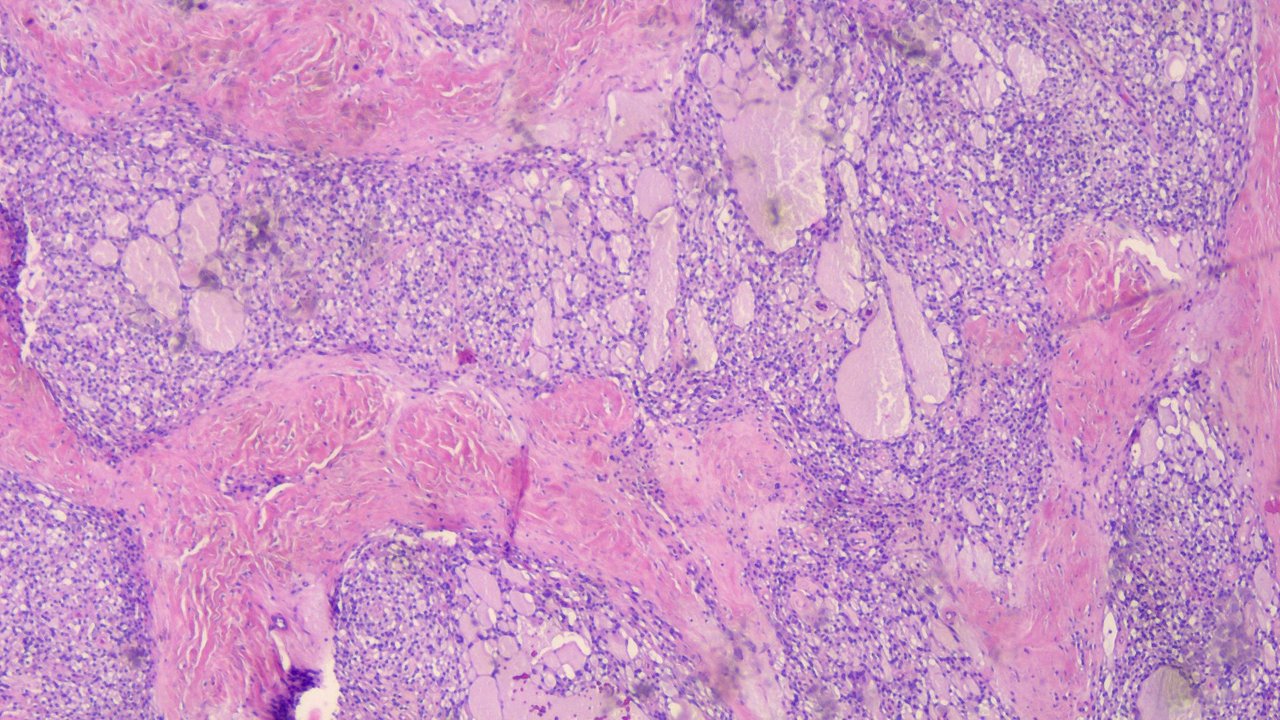
Taken at low power view (100x):
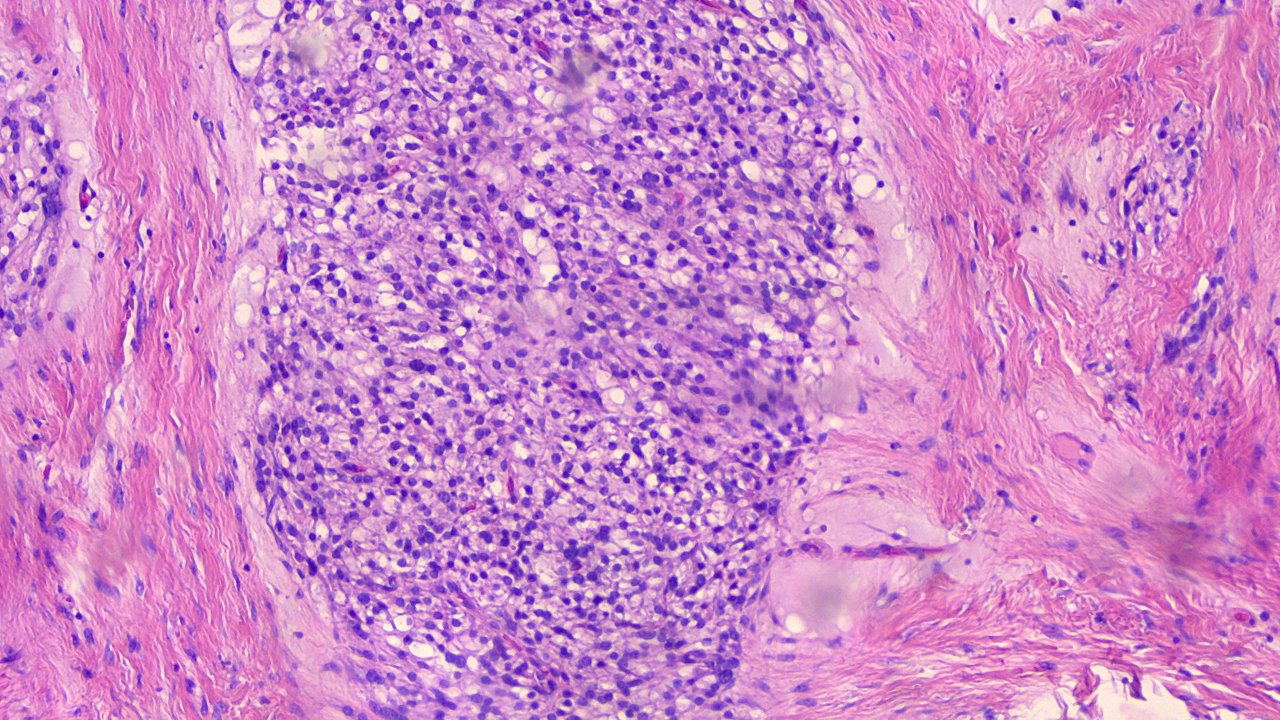
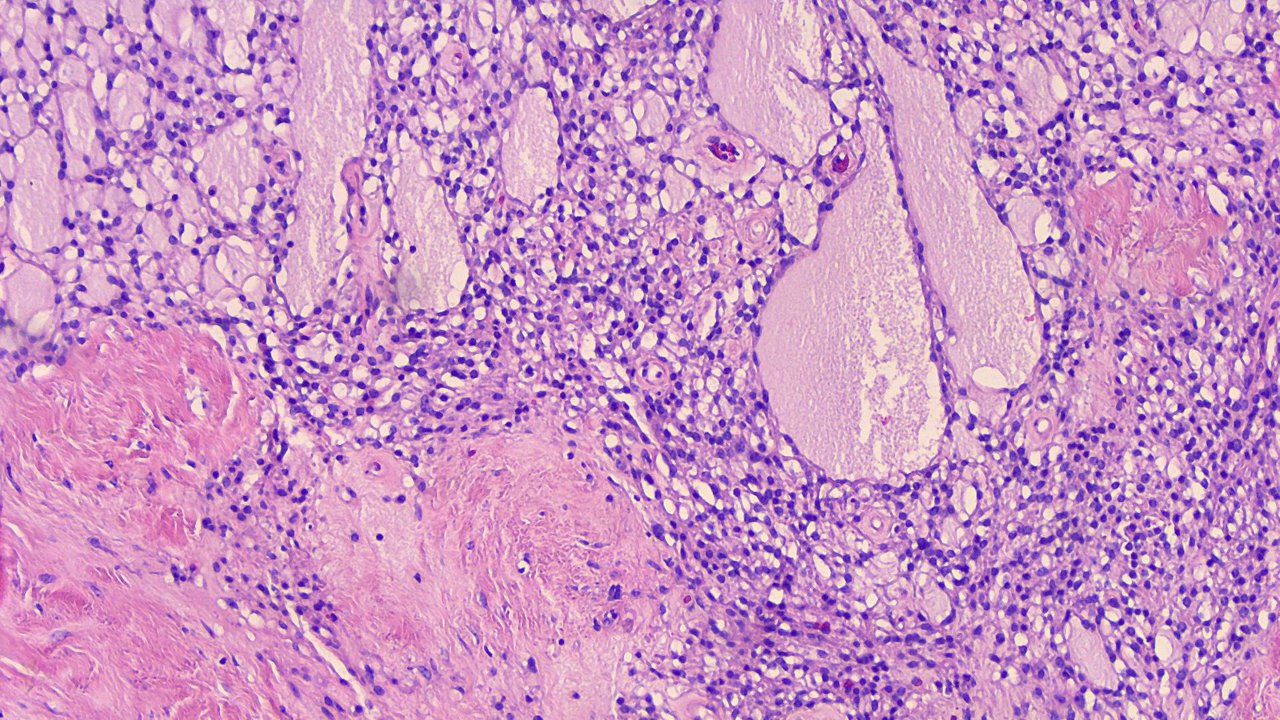
The solid cellular areas contain microcysts that coalesce to form channels on some parts. There's a clear demarcation between the nests of tumor cells from the intervening fibrous stroma.
Taken at high power view (400x):
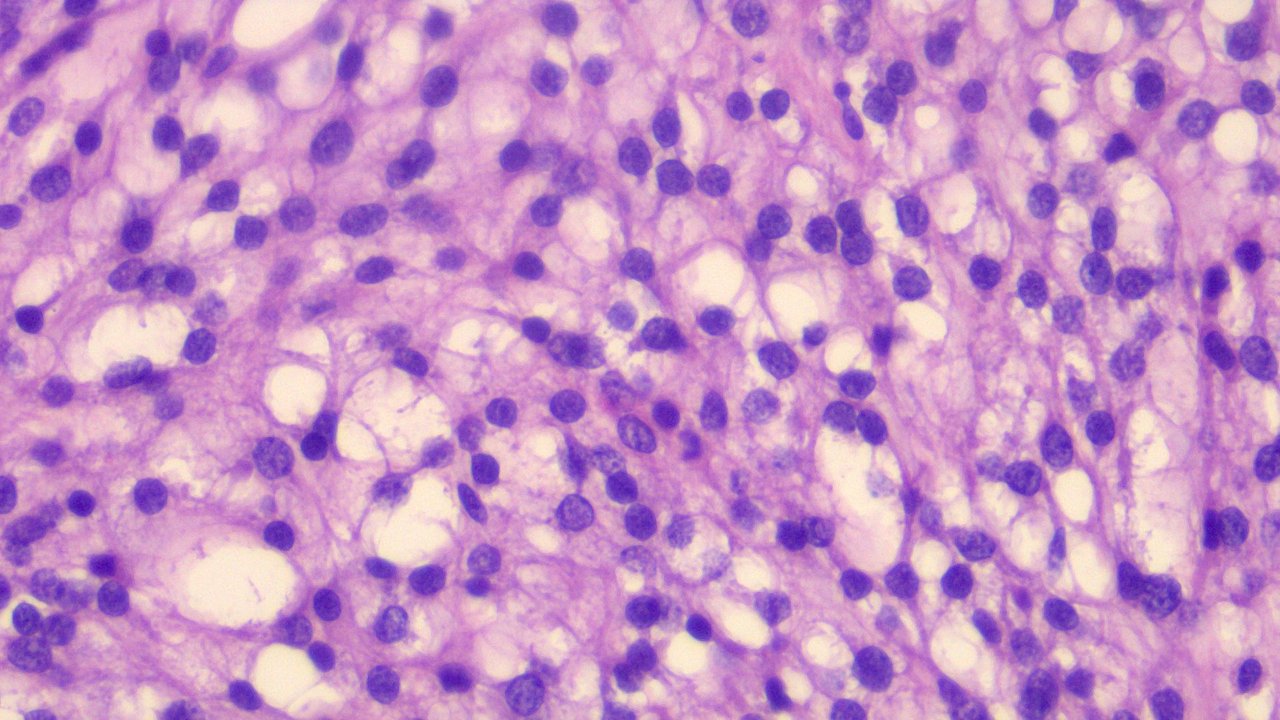
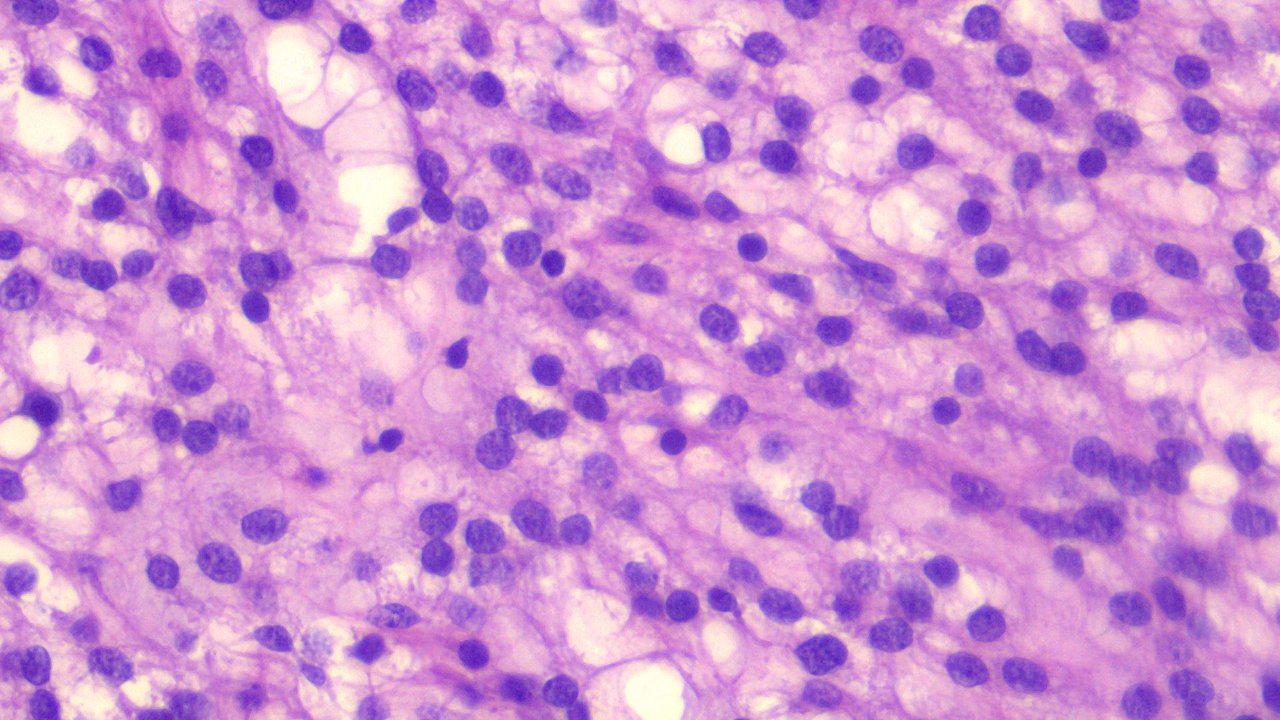
The tumor cells have round to oval, bland, hyperchromatic nuclei with inconspicuous nucleoli and granular ample eosinophilic cytoplasm. Mitotic activity here is low (malignant neoplasms tend to have high mitotic activities because these rapidly divide).
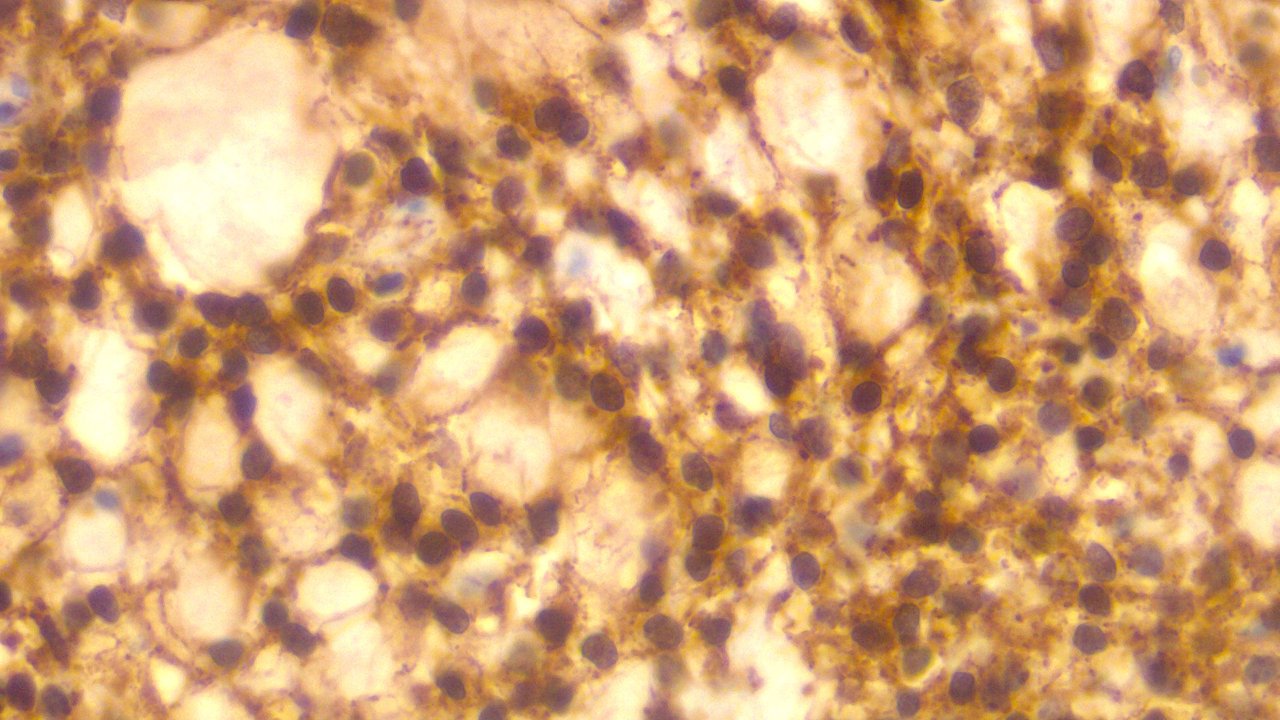
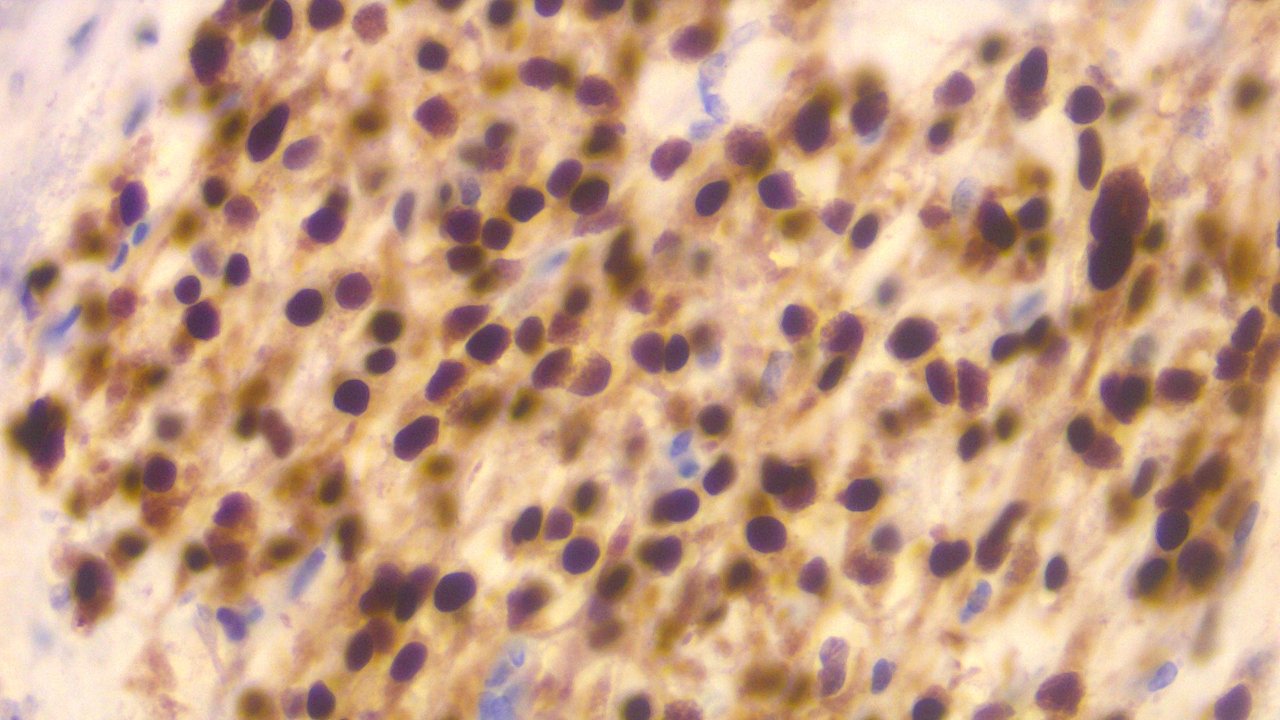
These are immunoreactive for Beta Catenin and Cyclin D1. They are negative for inhibin which rules out other sex cord stromal tumors that are malignant in origin.
Immunohistochemical studies are for aiding in diagnosis, ruling out other possible diagnosis, identifying the tumor origin, and prognostication.
Beta Catenin positive:
Cyclin D1 positive:
Inhibin Negative:
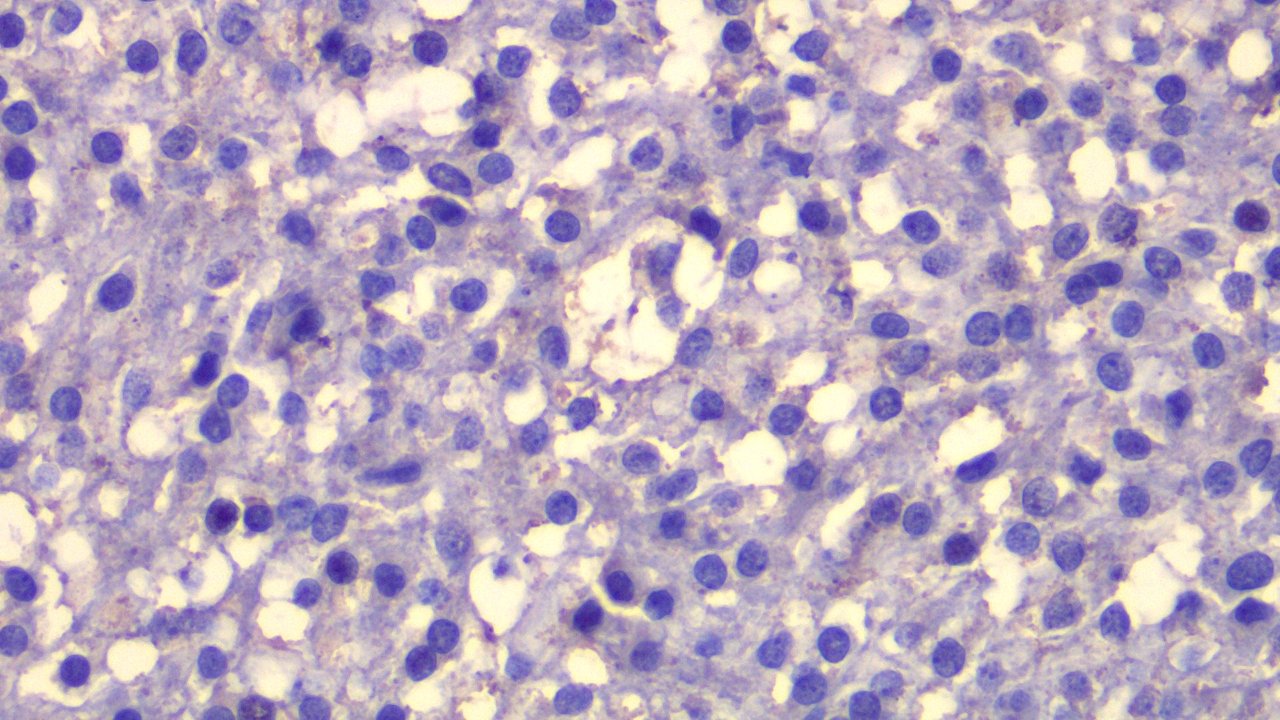
I can confidently sign this case out as Microcystic Stromal Tumor based on the morphologic findings alone but having immunohistochemical studies helps me sleep better at night. Because inhibin here is negative for staining, this rules out other malignancies possibly considered. The patient didn't had any prior biochemical markers for inhibin, beta HCG, and AFP so that didn't rule out other possible diagnosis.
I've seen cases when I'm confident about something based on morphology only for it to go 360 once the immunohistochemical studies were done. This case is benign.
Pathology is evolving towards the genetic and molecular level because some disease entities can't be diagnosed by just looking at the morphology when features between malignant and benign overlap. One thing I like about this case is that sense of accomplishment that I followed through it from grossing to immunohistochemical studies. Sometimes I only get to start at the initial parts of the case before someone else takes over and I didn't get to see the ending.
This being a not so common diagnosis made documenting fulfilling. It's not a case reportable level but if you're the type that enjoys academic trivia, these are one of those cases to note.
If you made it this far reading, thank you for your time.
Posted with STEMGeeks
Comments