A Case of Anaplastic Large Cell Lymphoma
2 comments
The number of cases since pandemic have picked up and once in a while I get complicated, and relatively rare interesting cases. When I tag a case as interesting, it really doesn't mean good news for the patient as it's usually entails poor prognostic outcomes.
I've already gave the spoiler to the diagnosis so the pictures below are just parts of the story. This came from a 27 year old male whom I'm been following up for the past few weeks. The specimen was a left thigh mass that was gradually ulcerating. Due to the graphic nature of the disease, I won't be sharing the gross parts.
They transferred to our institution because they felt that the other institution were delaying their care and they were really anxious to seek help. Other than trying to figure out what we're dealing with.
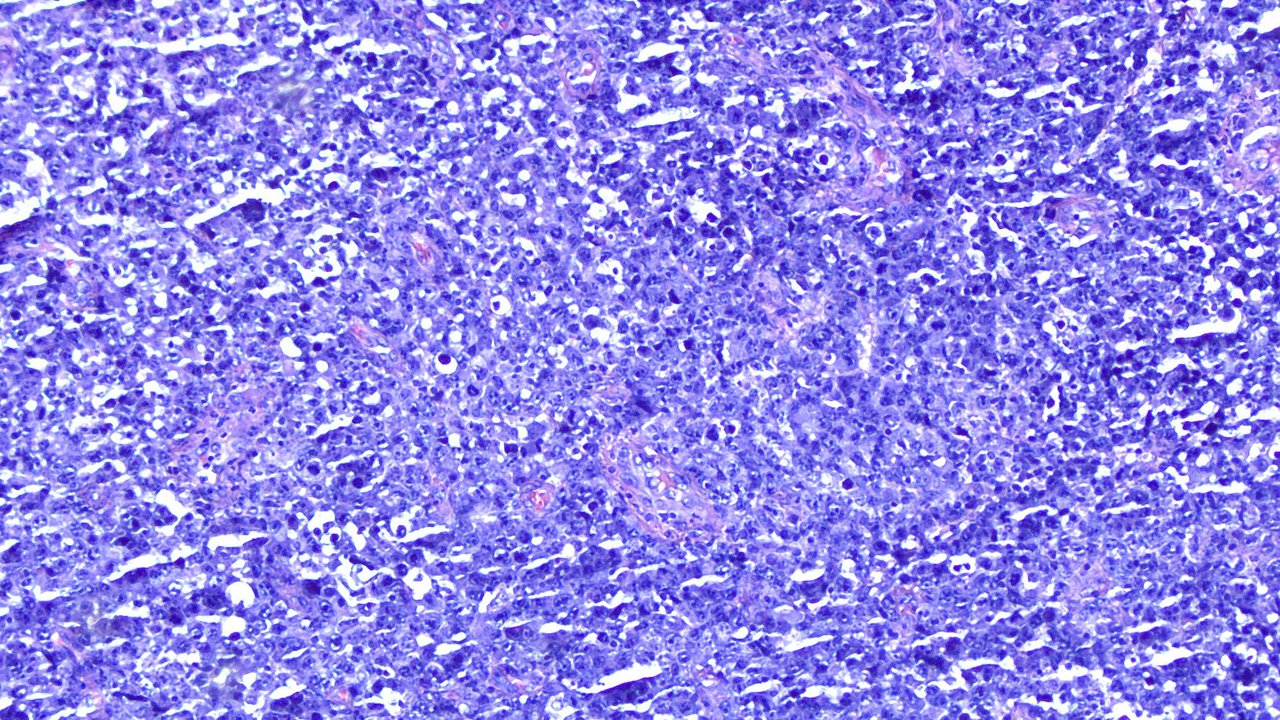
Here's image of the tumor at low power view:
And at high power view (400x):
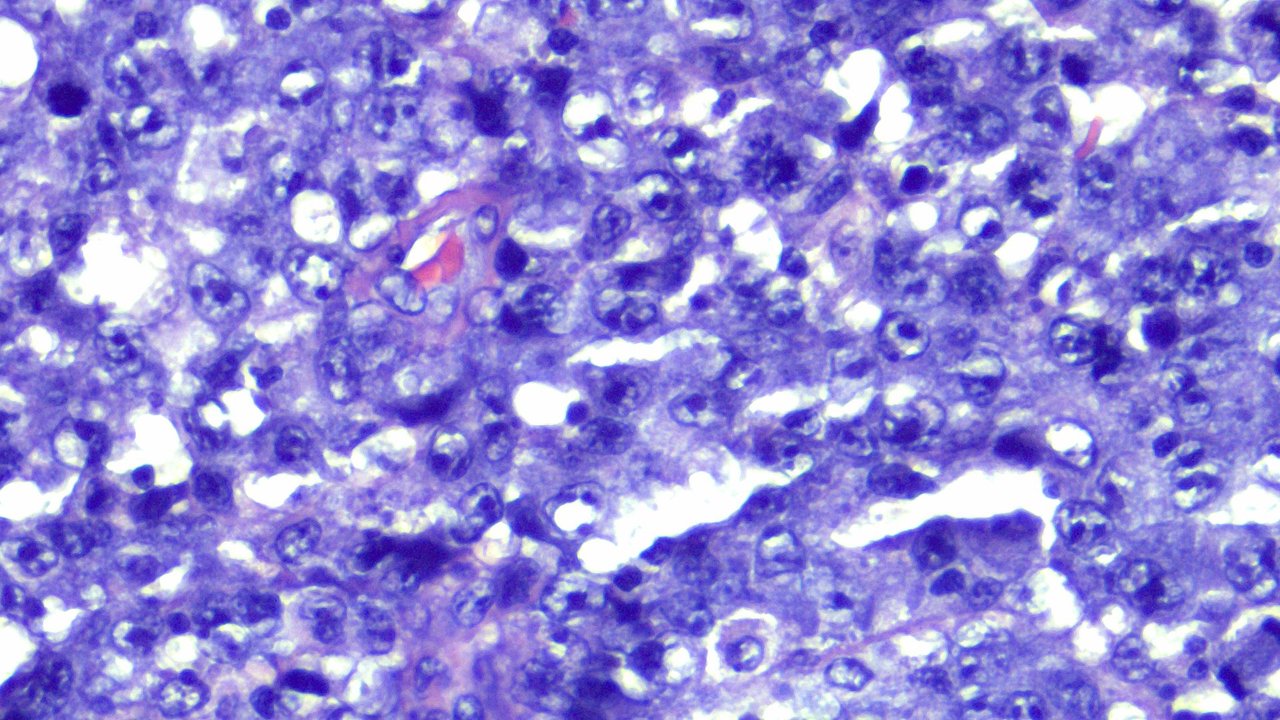
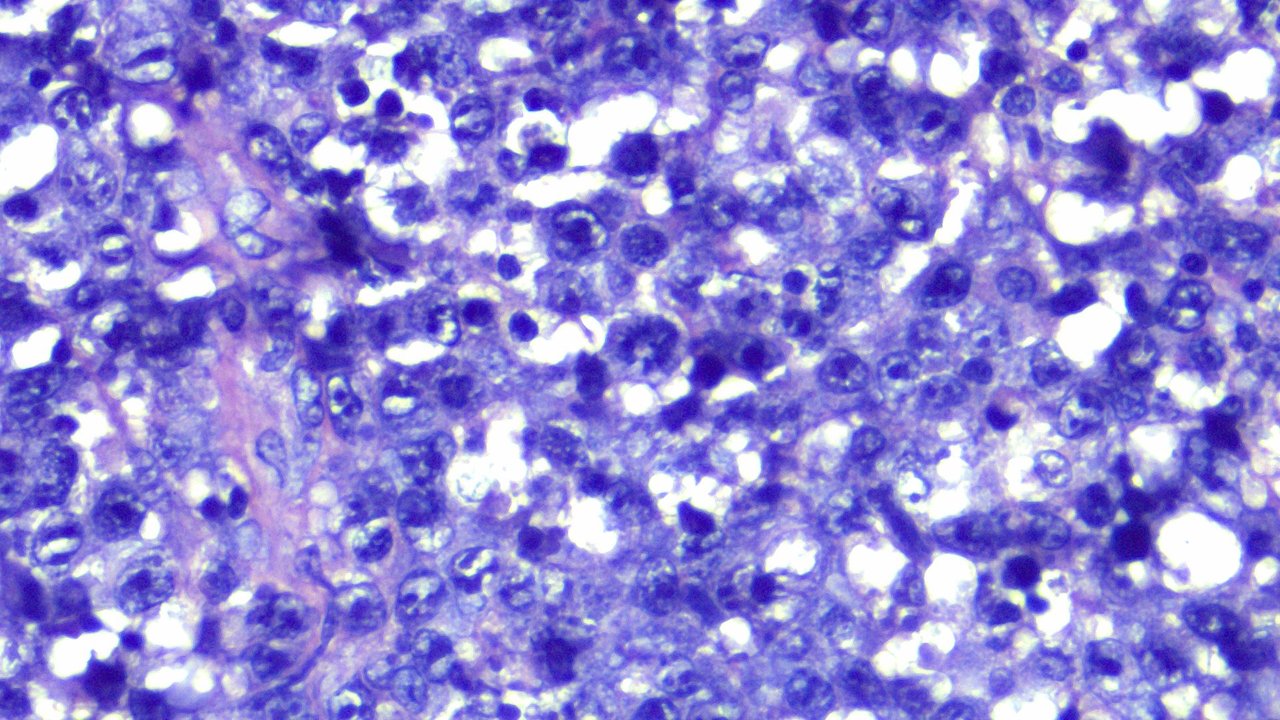
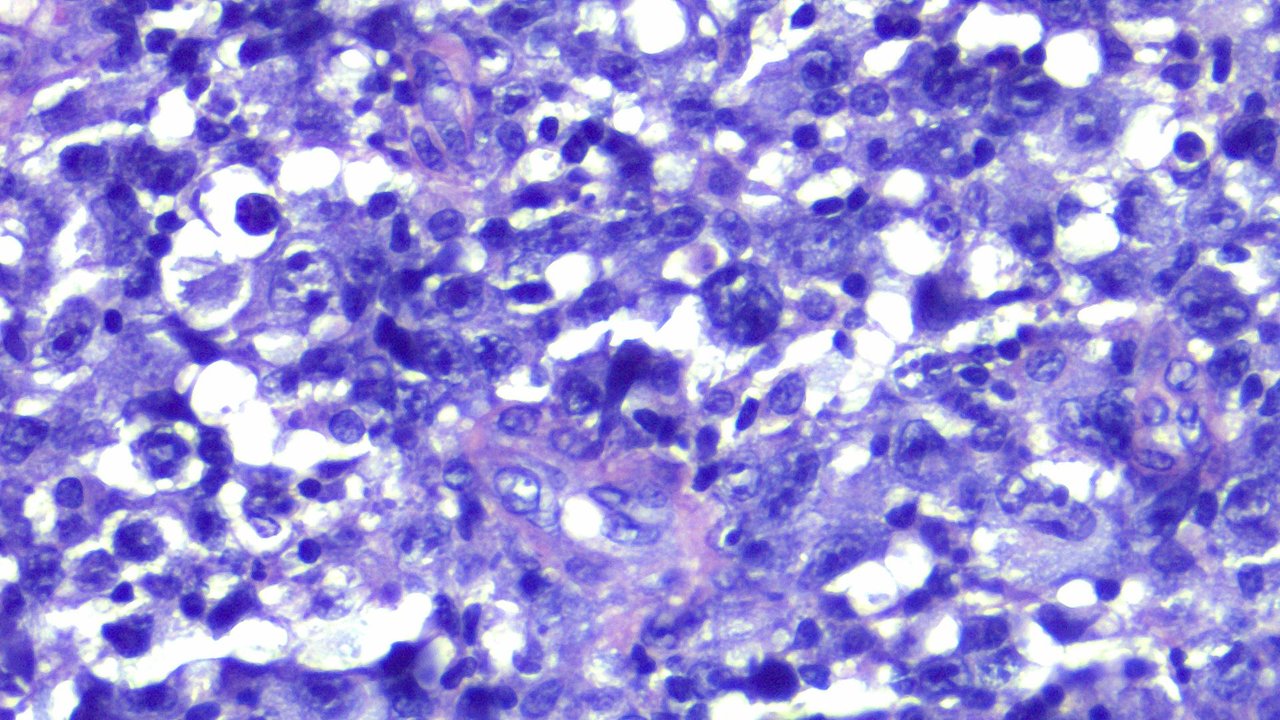
The cells don't look uniform, some are hyperchromatic to vesicular, markedly pleomorphic nuclei with inconspicuous to prominent nucleoli and moderate to abundant cytoplasm. You can see some of the actively dividing cells on these images.
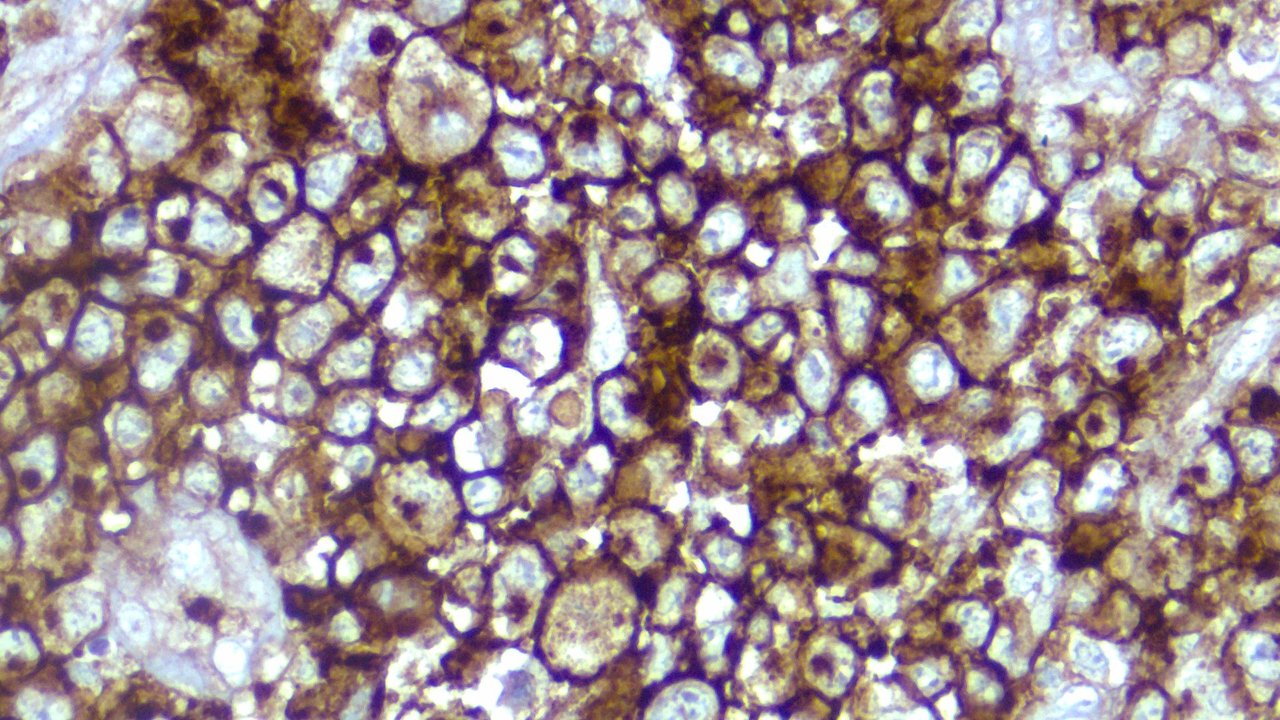
By morphology alone, this looks like a case of Melanoma, but given the site, Sarcoma needs to be ruled out. So a lot of special stains were requested to rule out sarcomas, carcinomas, and melanomas. When CD45 lit up:
CD45 is a marker for hematolymphoid cells, so this confirms the lineage to narrow it to lymphoma. You can see the bronw pigment highlighting the cell borders because tumore cells are positive for membranous expression.
Given the morphology, the differentials now were NOn-Hodgkin's Lymphoma vs Anaplastic Large Cell Lymphoma.
Now I won't go into academic details about how to differ each and what this means because that would stretch this post and bore. But for those who have an interest for medical stuff, you can look up the case as this isn't something often encountered.
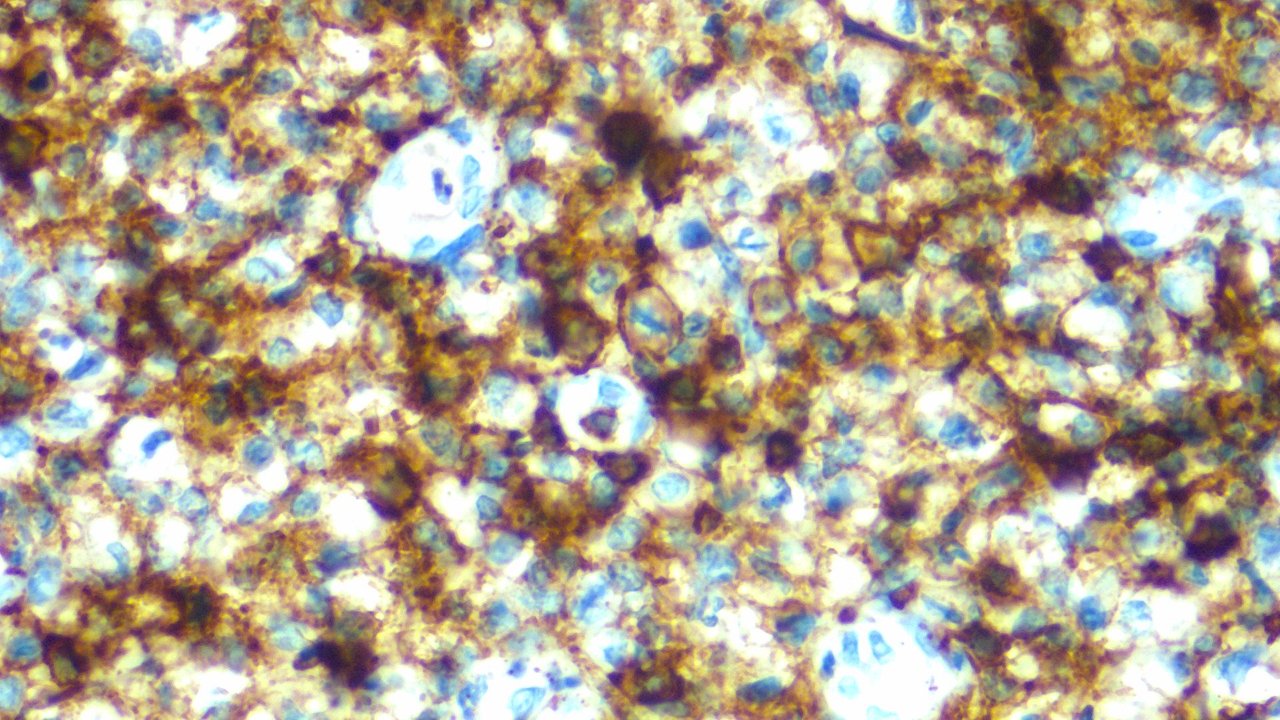
CD30 being positive helped supported an Anaplastic Large Cell lymphoma. Although this is also positive for Non-Hodgkin Lymphoma Large Cell types, combined with other stains, imaging and history we found it consistent with Anaplastic Large Cell.
CD30, like CD45 is expressed in tumor cells as a membranous stain.
Immunohistochemistry studies aren't cheap so we have to be selective about what we recommended. Only the most specific and needed stains will be recommended as much as possible. The problem arises when the results turn out inconclusive, so trying to do more stains in the first place would have saved up a week's time but we can't just order a battery of tests all the time. It's costly and generally unnecessary.
For rare reportable cases, this becomes an exception but delays that can span for weeks happen. It didn't help that the patient came from a far away place where phone signals are limited so I have to convince them to follow up at specific dates so as they can do the most out of their time within the city.
Of course the trouble of financial burdens arise and to make this part of the story short, I covered the remaining stains needed to clinch the diagnosis with them telling giving me an IOU. It was never paid back, the patient expired a few days ago.
The folks tried to make an effort to reach me personally and I was like, indirectly avoiding the contact. I don't need the excess baggage of gratitude or sad stories in my mental space but I do acknowledge that people need the chance to show their appreciation? anyway, it's only over through text did I receive the conclusion and it was through text that I just said they should not mind the debt and use it for the funeral expenses. It wouldn't help me sleep better at night if I took my money anyway.
I'm a bad story teller giving spoilers ahead. Sensationalizing things is just not my thing. The reason why this case adds to the list of the cases that changed my view about life and death is seeing the process of grief and anticipation. I've seen it before but I don't go actively look for it nor spend too much time minding it.
The formula is seeing them read the report you made and asking "is this cancer?" and the automated response is, this is really something you should be discussing with your main doctor as I don't want to overstep my boundaries. I would follow up with the most comforting and solution directing words like telling them which way to proceed next, what department and who to look for when they want to seek treatment. I said this many times and talked to different faces with the rhyming pain and suffering.
They mustered a smile but I didn't need to feel their internal world crumbling as I can see the overt welling of tears and trembling of their voices as they process the news. I'm sorry was all that I could say.
Anaplastic Large Cell Lymphoma has a poor prognosis especially if it's ALK negative.
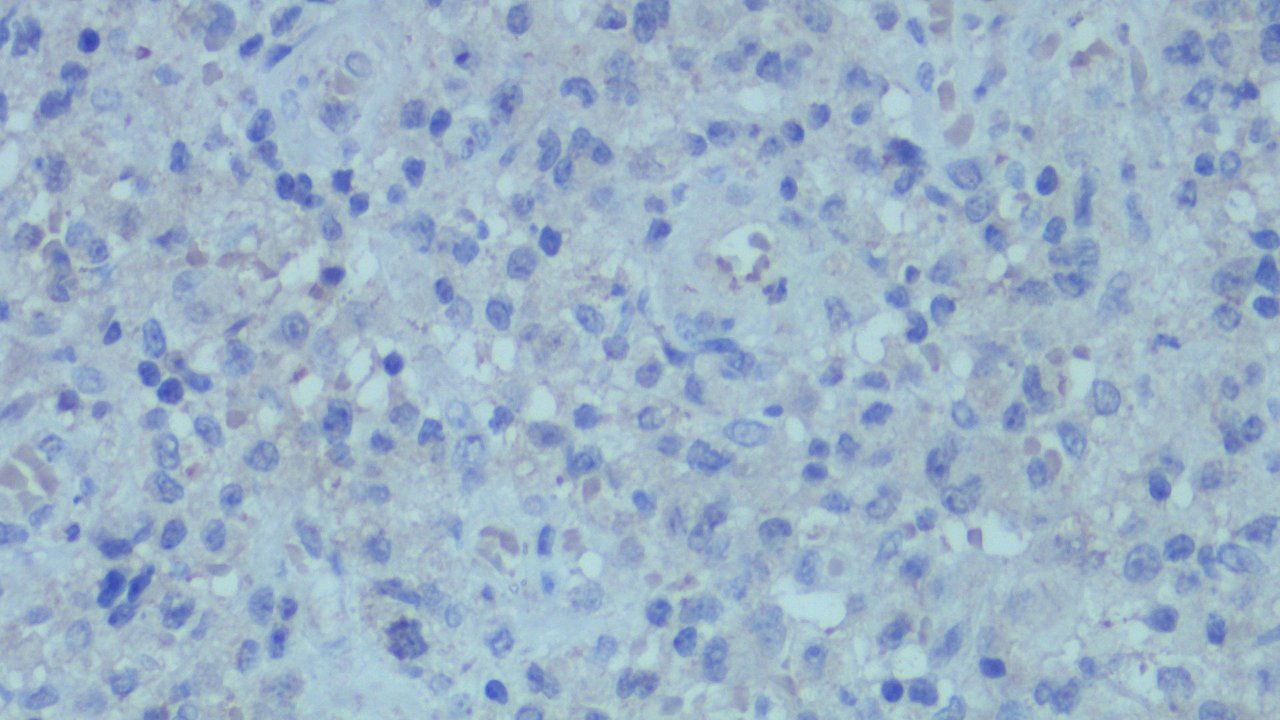
You can see the tumor cells not giving any brown pigments on their cytoplasm. The brownish tinged you see is only a background stain and not really valid because we need to see it clearly brown and highlighting the cells.
Other stains not shown but turned out negative were CK, Desmin, HMB45, S100, Melan A, CD3, CD20, and CD34. The ALK stain is for prognostication as ALK positivity has shown a favorable response to chemo. But on this case, the disease has already spread that the patient was too weak to carry the side effects.
If you made it this far reading, thank you for your time.
Posted with STEMGeeks
Comments